
How to justify psychiatric genetics
Does psychiatric genetics make sense, given what conceptions of the nature of psychiatric phenomena does it make sense?

Eiko Fried is one of my favorite psychological scientists to agree with. He is sharp, reasonable, well-read, and diligent. If he is on your side (there are no sides), he will at some point lay out the argument so well that little remains to be said. This is also why he is my favorite psychological scientist to disagree with. He makes you work for it. In the process of overthinking one of his papers, tweets, or blog posts, you come away with a far better articulation of your position than you thought you would have. He doesn't just live rent-free in my mind; he is the mayor of a cute mid-size German town in there, like they have a tram. I have had the privilege of meeting up with him IRL for coffee and a frantic hour and a half of shop talk, an invigorating and valuable experience (@Eiko, let's do this again soon!).
Yesterday, he reacted to (well, quote tweeted, so low stakes) a press release announcing increased philanthropic funding for genetics research into bipolar disorder. The press release announces funding for two things. First, there is funding for sequencing patients with a bipolar disorder diagnosis and their unaffected relatives or screened controls who do not have bipolar disorder across the globe. The second part of the funding goes to sequencing the genes expressed or regulated in a certain way in individual cells sampled (post-mortem) all across the brains of people who lived with bipolar disorder and those that did not. Full disclosure: I have worked with or currently work with some of the people involved but am not involved in this work myself.
He specifically asked what we need to assume about the nature of bipolar disorder to make this investment worthwhile. I'll happily oblige and lay out what we assume about psychiatric disease for the first research goal to be worthwhile: "nothing".


"Nothing" is the kind of answer that either needs to be deeply motivated, or I need to step aside and let the grown-ups handle the science. So let me attempt to motivate it.
Medical, biological, and social sciences (I consider psychiatric phenomena as "at home" in all three) rely on the ability to infer cause and effect with a reasonable degree of certainty. The definition of "reasonable" varies greatly across domains, but a general rule, in my opinion, is that further increasing certainty would be prohibitively expensive, unethical, or otherwise unreasonable. To achieve this, people perform controlled experiments. However, when studying the causes of psychopathology, ethical limits quickly become apparent.
For example, to determine whether staying up late increases the risk of mania or manic episodes, one could experiment with an intervention that motivates people to go to bed early and get plenty of rest. However, it's not feasible to deprive people with bipolar disorder or bipolar risk of sleep for long periods for obvious reasons. While there are many experimental options for cells or systems in biology, it's difficult to link those interventions to bipolar disorder in humans without going through a chain of experiments in animal models. Unfortunately, animal models of psychiatric diseases aren't ideal, to my mind most are implausible as models, and they have obvious ethical issues.
In general, while experiments may work within psychology/medical sciences and within biology, linking biology to behaviour from a causal inference perspective is very VERY challenging.
When experiments aren't feasible, the next best thing is to use pseudo or natural experiments, as well as a range of causal inference techniques. For instance, if we want to determine whether staying up a little later triggers mania, we could follow people as they go through daylight savings or jet lag and compare their outcomes to previous periods in their life or to matched controls. There are several well-designed and controlled pseudo-experimental studies that provide clear examples of this approach. Consider work by Ken Kender et al. who contrasted (sexually) abused to un-abused siblings in terms of later psychiatric outcomes1, work that contrasts Swedish survivors of the 2004 Christmas day tsunami to unaffected Swedes in terms of traumatic responses2 and pathologies3 and finally work that tries to establish whether neighbourhood density increases risk for schizophrenia, but does so within siblings to control for al manner of confounding4. I think most would agree these kinds of study designs have flaws that make them less then perfect substitutes for experiments, but they certainly further our understanding of psychological response to exposures we cant experiment with easily.
It may appear that we don't have clear-cut, observable exogenous contrasts available to test whether specific biological processes cause complex psychiatric phenomena. Except that we do: genetics. The primary use of genetics is to link exposures (usually biology, but not always) to distant outcomes (can be anything). For example, if we suspect that a hypothetical cellular process called "neural dendrite differentiation" (NDD) is always slowed down in people who develop bipolar disorder, then a gene that slows down NDD will increase the risk of bipolar disorder. To test this, we could look for/at that specific gene in isolation, but doing genetics right requires three things: large samples, coherent uniform evaluation of all genes, and a tightly controlled type 1 error rate.
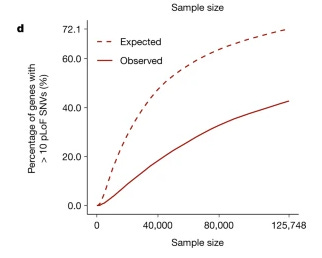
Therefore, it makes sense to seek out genes related to bipolar disorder at scale and well. The funding announced here is primarily meant for the detection of rare variants with significant effects, which means it's crucial to seek out samples across the globe.The kind of rare variant that severely inhibits, or blocks the function of a gene is selected against if its very debilitating5. These rare, somewhat debilitating genetic variants won't become common enough to be found in populations across the globe. Instead, if these variants arise through mutation, they will cause slight harm to someone, their children, and grandchildren. However, depending on the level of impact and selection against the variant, it won't become prevalent. Some scientists keep track of how often we see a variant that knocks out or severely inhibits a gene in all of our collective data, and it's actually quite rare. In 125,000 sequences of people, about 40% of genes have at least ten individuals who carry a broken copy.
It is feasible, but hard, to figure out for each gene whether it relates to bipolar disorder, and than trace back trough biological experiments what systems, cells, processes break down if these genes malfunction. Genes are one of the rare viable causal threads that can link biology to psychiatry. Which means that they are also one of the rare causal threads to rule out a link between a specific biological process and psychiatry. In fact to date most of the useful applied examples of genetics in psychiatry has been about ruling out hypothesis. How do we as a field proceed when we observe a relation between vitamin-D and depression? One option is to run a $12M randomised controlled trial (and they did, only to find no effect whatsoever6), or you could find out whether genetic variants that relate to circulating levels of Vitamin-D, also relate to depression (you'd expect them to if vit-d causes depression, but they don't7) and save a buck.
Genes, and genetic effects, apart from the rare cases they directly point to an actional disease phenotype, are most effective when used as agnostic causal anchors. On these causal anchors we can scaffold better theory and models linking biology to psychiatry, or rejecting those links. Genetics of psychiatric outocome is in principle usefull regardless of the nature of psychiatric phenomena, and in fact I think it can aid us understand psychiatric phenomena far better. This post has an obvious positive spin on the use of genetics in psychiatry as I am trying to make the case for it. The actual science is hard, has various limits, requires assumptions. There are serious challenges in terms of phenotyping, measurement, and bias, but on the whole psychiatric genetics is certainly a worthwhile effort.
Kendler, K. S., Bulik, C. M., Silberg, J., Hettema, J. M., Myers, J., & Prescott, C. A. (2000). Childhood sexual abuse and adult psychiatric and substance use disorders in women: an epidemiological and cotwin control analysis. Archives of general psychiatry, 57(10), 953-959.
Johannesson, K. B., Michel, P. O., Hultman, C. M., Lindam, A., Arnberg, F., & Lundin, T. (2009). Impact of exposure to trauma on posttraumatic stress disorder symptomatology in Swedish tourist tsunami survivors. The Journal of nervous and mental disease, 197(5), 316-323.
Arnberg, F. K., Gudmundsdóttir, R., Butwicka, A., Fang, F., Lichtenstein, P., Hultman, C. M., & Valdimarsdóttir, U. A. (2015). Psychiatric disorders and suicide attempts in Swedish survivors of the 2004 southeast Asia tsunami: a 5 year matched cohort study. The Lancet Psychiatry, 2(9), 817-824.
Sariaslan, A., Larsson, H., D’Onofrio, B., Långström, N., Fazel, S., & Lichtenstein, P. (2015). Does population density and neighborhood deprivation predict schizophrenia? A nationwide Swedish family-based study of 2.4 million individuals. Schizophrenia Bulletin, 41(2), 494-502.
Karczewski, K. J., Francioli, L. C., Tiao, G., Cummings, B. B., Alföldi, J., Wang, Q., ... & MacArthur, D. G. (2020). The mutational constraint spectrum quantified from variation in 141,456 humans. Nature, 581(7809), 434-443.
Okereke, O. I., Reynolds, C. F., Mischoulon, D., Chang, G., Vyas, C. M., Cook, N. R., ... & Manson, J. E. (2020). Effect of long-term vitamin D3 supplementation vs placebo on risk of depression or clinically relevant depressive symptoms and on change in mood scores: a randomized clinical trial. Jama, 324(5), 471-480.
Milaneschi, Y., Peyrot, W. J., Nivard, M. G., Mbarek, H., Boomsma, D. I., & WJH Penninx, B. (2019). A role for vitamin D and omega-3 fatty acids in major depression? An exploration using genomics. Translational psychiatry, 9(1), 219.